The UK Marine Accident Investigation Branch (MAIB) has published an accident investigation report into a fatal crush incident during lifting operations on the general cargo vessel Karina C
What happened?
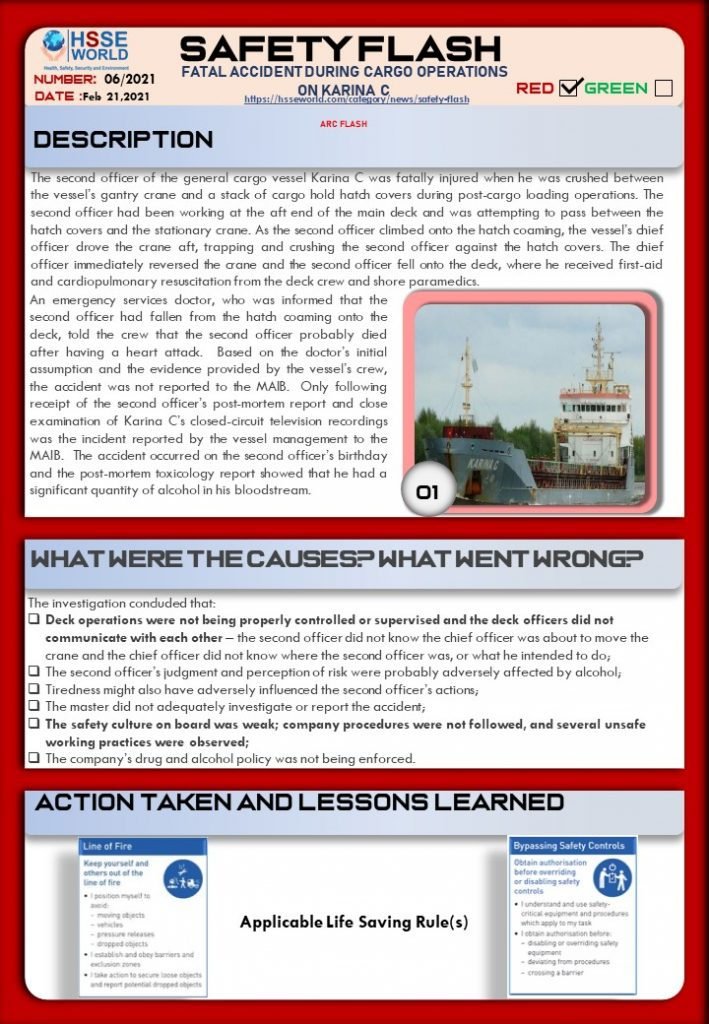
The second officer of the general cargo vessel Karina C was fatally injured when he was crushed between the vessel’s gantry crane and a stack of cargo hold hatch covers during post-cargo loading operations.

The second officer had been working at the aft end of the main deck and was attempting to pass between the hatch covers and the stationary crane. As the second officer climbed onto the hatch coaming, the vessel’s chief officer drove the crane aft, trapping and crushing the second officer against the hatch covers. The chief officer immediately reversed the crane and the second officer fell onto the deck, where he received first-aid and cardiopulmonary resuscitation from the deck crew and shore paramedics.
An emergency services doctor, who was informed that the second officer had fallen from the hatch coaming onto the deck, told the crew that the second officer probably died after having a heart attack. Based on the doctor’s initial assumption and the evidence provided by the vessel’s crew, the accident was not reported to the MAIB. Only following receipt of the second officer’s post-mortem report and close examination of Karina C’s closed-circuit television recordings was the incident reported by the vessel management to the MAIB. The accident occurred on the second officer’s birthday and the postmortem toxicology report showed that he had a significant quantity of alcohol in his bloodstream.
What went wrong
The investigation concluded that:
- Deck operations were not being properly controlled or supervised and the deck officers did not communicate with each other – the second officer did not know the chief officer was about to move the crane and the chief officer did not know where the second officer was, or what he intended to do;
- The second officer’s judgment and perception of risk were probably adversely affected by alcohol;
- Tiredness might also have adversely influenced the second officer’s actions;
- The master did not adequately investigate or report the accident;
- The safety culture onboard was weak; company procedures were not followed, and several unsafe working practices were observed;
- The company’s drug and alcohol policy was not being enforced.
you can download the Safety Flash by clicking download below
These flashes summarise key safety matters and incidents, allowing wider dissemination of lessons learned from them. The information below has been provided in good faith by members and should be reviewed individually by recipients, who will determine its relevance to their own operations. The effectiveness of the safety flash system depends on receiving reports from members in order to pass on the information and avoid repeat incidents.
Source and download
| Alert ID: | 06/21 |
| Published: | Feb 16 2021 |
| Download: | Safety flash (333 kB) |
Read More Safety Flash
- Safety Flash: Mobile concrete placing boom overturn incidents
- Safety Flash: Not Following Work permit and Isolation Procedure
- Safety Flash: Floorman arm pinned by Pipe Handling Equipment
- Safety Flash: Suspension Trauma
- Safety Flash: Fatality: explosive failure of corroded fire extinguisher
- Safety Flash: Crewman fell to his death through faulty grating
- Safety Flash: Fatal accident during cargo operations on Karina C
- Safety Flash: Overturning of the Lifeboat Kristin Faye
- Safety Flash: Short circuit on 440v AC bus bars-arc flash
- Safety Flash: Towing Fatality
- Safety Flash: Unsafe lifting operations
- Safety Flash: Electric Shock Resulting in Burn
- Safety Flash: LTI- Loss of Finger Tip and Nail
- Safety Flash: Explosion And Fire Onboard The chemical Tanker STOLT Greenland
- Safety Flash: Finger injury caused by incorrectly secured console cover
- Safety Flash: double Man overboard Resulting in one fatality
- Safety Flash: Alcohol-based hand sanitizer warning
- Safety Flash: Dump truck operator fatally electrocuted by high-voltage line
- Safety Flash: Laborer Dies After Footing Collapse – North Carolina
- Safety Flash: Reducing the risk of propane explosions in food trucks
- Safety Flash: Teen Roofer Electrocuted when Ladder Contacts High Voltage Power Line
- Safety Flash: Worker dies from carbon monoxide poisoning while using pressure washer
- Safety Flash: Explosion during welding operation
- A Bathtub Refinisher Dies from Methylene Chloride Exposure :Safety Flash
- Landscaper dies after auger entanglement:Safety Flash
- Worker dies after falling from scaffold
- Fatality Investigation: Orchard Worker Dies After Falling Off Tractor
- LTI: Fall from height leading to Multiple Fractures
- Operator dies when forklift falls off loading dock
- Worker struck, killed by outrigger
- Worker killed by platform
- Scaffolding Components
- Construction Worker Killed When Pipe Rolls Off a Trailer
- Near-Miss: Shackle Configuration
- Improper use of lifeline results in death of worker